

Description: The maternal mortality ratio (MMR)[1] (188) can give an indication of the gender sensitivity of the health system. This indicator together with the adolescent birth rate (ABR) are used to calculate the reproductive health contribution of the Gender Inequality Index.
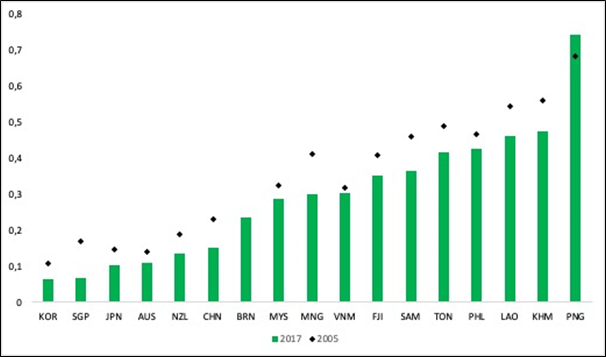
The maternal mortality ratio (MMR)[1] (188) can give an indication of the gender sensitivity of the health system given the MMR together with the adolescent birth rate (ABR) are the two indicators used to calculate the reproductive health contribution of the Gender Inequality Index (see Figure 1).
Figure 1: Gender Inequality Index, selected countries, Western Pacific Region, 2017 (34)
While the maternal mortality ratio has improved substantially in all countries since 2000 it has also plateaued in all countries, for many from 2010 onwards (189). For women in Papua New Guinea, Lao PDR and Cambodia maternal mortality rates remain quite high at 215, 197 and 161 deaths per 100 000 live births respectively (2015) (see Table 4). Despite improvements in areas such as antenatal care (ANC) at least one visit, first available data from 2000 compared to the last reported data suggests that progress is not always sustained. For example, ANC one visit coverage has decreased from 100% in Kiribati and Palau to 88.4% and 90.3% respectively, and in Vanuatu from 84.3% to 75.6%. However last reported data in the three countries was 2009 (Kiribati), 2010 (Palau) and 2013 (Vanuatu).
As indicated previously education is a key determinant of health for both men and women. Figure 14 illustrates how in countries where a higher percentage of the female population have at least some secondary education, the MMR is considerably lower and in countries such as PNG with the highest MMR, less than 20% of the female population have some secondary education (35,189,190). It also potentially highlights points of intervention for different countries such as Tonga and the Philippines where the MMR is above 100 but at least 75% of the female population have some secondary education. Here reducing the MMR might be linked to strengthening the AAAQ of services and care such as ensuring access to appropriate ANC and skilled birth attendance. The relatively high MMR in these and other countries with good levels of secondary education among females may also reflect in-country inequities based on education, wealth quintile, ethnicity and or place of residence (rural/urban) linked to the AAAQ of health services and care.
Table 4. Maternal mortality ratio, Adolescent Birth Rate, and Satisfaction with modern methods of contraception, selected countries, Western Pacific (188,189,191,192)
| MMR 2015 | ABR 2015 | Satisfied with modern methods (%) 2007-2014 | |
| Australia | 6.0 | 11.9 | – |
| Brunei Darussalam | 23.0 | 11.4 | – |
| Cambodia | 161.0 | 57.0 | 56.4 |
| China | 27.0 | 9.2 | – |
| Fiji | 30.0 | – | – |
| Japan | 5.0 | 4.1 | – |
| Kiribati | 90.0 | 49.9 | 35.8 |
| Lao People’s Democratic Republic | 197.0 | 75.6 | 61.3 |
| Malaysia | 40.0 | 11.5 | – |
| Marshall Islands | – | – | 80.5 |
| Micronesia (Federated States of) | 100.0 | – | – |
| Mongolia | 44.0 | 26.7 | 68.3 |
| New Zealand | 11.0 | 16.0 | – |
| Papua New Guinea | 215.0 | – | 40.6 |
| Philippines | 114.0 | 57.0 | 51.5 |
| Republic of Korea | 11.0 | 1.3 | – |
| Samoa | 51.0 | 39.2 | 39.4 |
| Singapore | 10.0 | 2.7 | – |
| Solomon Islands | 114.0 | 42.0 | 38 |
| Tonga | 124.0 | 30.0 | 47.9 |
| Vanuatu | 78.0 | 78.0 | 50.7 |
| Viet Nam | 54.0 | 30.1 | 69.7 |
[1] The MMR represents the risk associated with each pregnancy, i.e. the obstetric risk and monitors deaths related to pregnancy and childbirth. The MMR reflects the capacity of the health systems to provide effective health care in preventing and addressing the complications occurring during pregnancy and childbirth.
References
Feedback




