

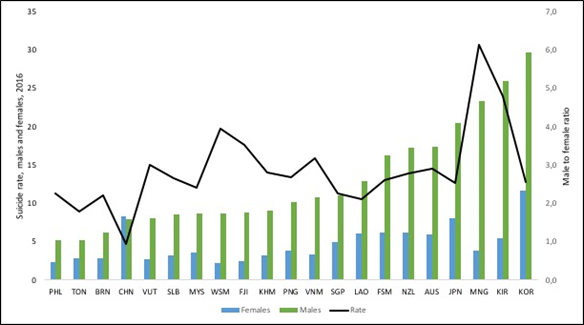
Age-standardized suicide mortality rates are the other NCD indicator in the UHC and SDG country profiles. They illustrate a well-known pattern that suicide mortality rates for men are consistently higher compared to women (Figure 11), with the exception being China where the rate is slightly higher among females (133). Suicide is an example of how men’s health may be affected by their (gender) roles and responsibilities. An Australian study found that men in male-dominated occupations had a rate ratio (RR) of 7.50 (95%CI 6.07 to 9.25) compared to males in female-dominated occupations indicating that the gendered context of an occupation influences suicide, with varying risks for women and men (134). Despite this, men are less likely to seek care and less likely to be diagnosed for disorders such as depression and receive appropriate care – reflecting gender norms and stereotypes both by men and among providers about men’s emotionality and expectations around coping (135).
Age standardized suicide rates (per 100,000 population), (SDG target 3.4.2) males and females, selected countries, Western Pacific Region, 2016 (133)
Depressive disorders however are a leading cause of DALYs for women in the Region (see Figure 6),
igure 6. Estimation of leading causes of DALYs in men and women, all ages, Western Pacific Region, 2016 (71)
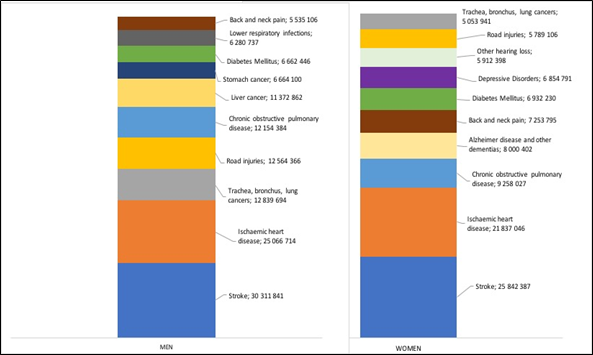
and globally women are two to four times more likely to attempt suicide than men (135).
Among men and among women, suicide rates are also high among groups who experience discrimination, such as refugees and migrants; indigenous peoples; lesbian, gay, bisexual, transgender, intersex (LGBTI) persons; and prisoners (136).
These differing patterns in NCD risk factors between men and women and among men and among women within countries highlight the need for gender analysis of sex- and age-disaggregated data cross linked with other data disaggregated by socioeconomic and cultural factors within countries to identify specific patterns relevant to country context and to support analysis of progress towards leaving no one behind.
References
Feedback




